Albring JC, Sandau MM, Rapaport AS, Edelson BT, Satpathy A, Mashayekhi M, Lathrop SK, Hsieh CS, Stelljes M, Colonna M, Murphy TL, Murphy KM.
Journal of Experimental Medicine, 22 November 2010
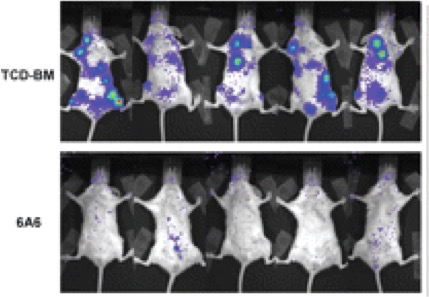
Graft-versus-host disease (GVHD) causes significant morbidity and mortality in allogeneic hematopoietic stem cell transplantation (aHSCT), preventing its broader application to non-life-threatening diseases. We show that a single administration of a nondepleting monoclonal antibody specific for the coinhibitory immunoglobulin receptor, B and T lymphocyte associated (BTLA), permanently prevented GVHD when administered at the time of aHSCT. Once GVHD was established, anti-BTLA treatment was unable to reverse disease, suggesting that its mechanism occurs early after aHSCT. Anti-BTLA treatment prevented GVHD independently of its ligand, the costimulatory tumor necrosis factor receptor herpesvirus entry mediator (HVEM), and required BTLA expression by donor-derived T cells. Furthermore, anti-BTLA treatment led to the relative inhibition of CD4(+) forkhead box P3(-) (Foxp3(-)) effector T cell (T eff cell) expansion compared with precommitted naturally occurring donor-derived CD4(+) Foxp3(+) regulatory T cell (T reg cell) and allowed for graft-versus-tumor (GVT) effects as well as robust responses to pathogens. These results suggest that BTLA agonism rebalances T cell expansion in lymphopenic hosts after aHSCT, thereby preventing GVHD without global immunosuppression. Thus, targeting BTLA with a monoclonal antibody at the initiation of aHSCT therapy might reduce limitations imposed by histocompatibility and allow broader application to treatment of non-life-threatening diseases.